
Issue Brief by Policy Analyst, Erin Twomey Partin | etpartin@csg.org
DOWNLOADWhat is Elder Abuse?
As the U.S. population ages, policymakers increasingly face challenges related to protecting older adults from abuse, neglect, and financial exploitation. There is no singular definition for elder abuse; different agencies and jurisdictions describe the qualifications for elder abuse in different ways. For the purpose of this issue brief, elder abuse is defined as an intentional or negligent act by any person that causes harm or a serious risk of harm to an older adult (aged 60 and older).1 Elder abuse can be further categorized into five groups (Table 1):2
Table 1. Types of Elder Abuse
| Psychological/Emotional | The infliction of anguish, pain, or distress on an older person through verbal or nonverbal acts or communication. Examples: Verbal aggression, social isolation, psychological torment, restricting access to assistive equipment |
| Physical | The infliction of pain or bodily harm on an older person that may result in injury. Examples: Pushing, hitting, unnecessarily forceful restraint |
| Neglect/Abandonment | The intentional denial of physical or emotional needs to an older person. Examples: Withholding food, denying healthcare, isolating |
| Sexual | Forcing sexual contact or engagement in sexual activity without consent. Examples: Forcing someone to watch sexual activity, sexual assault |
| Financial | The illegal or improper use of an older person’s money, property, or assets. Examples: Coercive behaviors that result in the elderly person giving away belongings, forgery, or theft. |
It is difficult to accurately predict the prevalence of elder abuse due to underreporting. However, the World Health Organization estimates that approximately 1 in 6 adults aged 60 and older globally experience some form of abuse each year.3 This abuse is often perpetrated by a trusted individual, with 46.8 percent of reported cases committed by a family member of the victim.4 Psychological or emotional abuse is the most reported type of elder abuse, with 67 percent of victims in reported cases being women.5 There is also some evidence that suggests victims experience multiple forms of abuse simultaneously.6
Though elder abuse affects older adults in both rural and urban areas, a study published in 2025 found that reported cases are more common in urban settings. However, elder abuse in rural communities may be less visible due to higher levels of underreporting.7
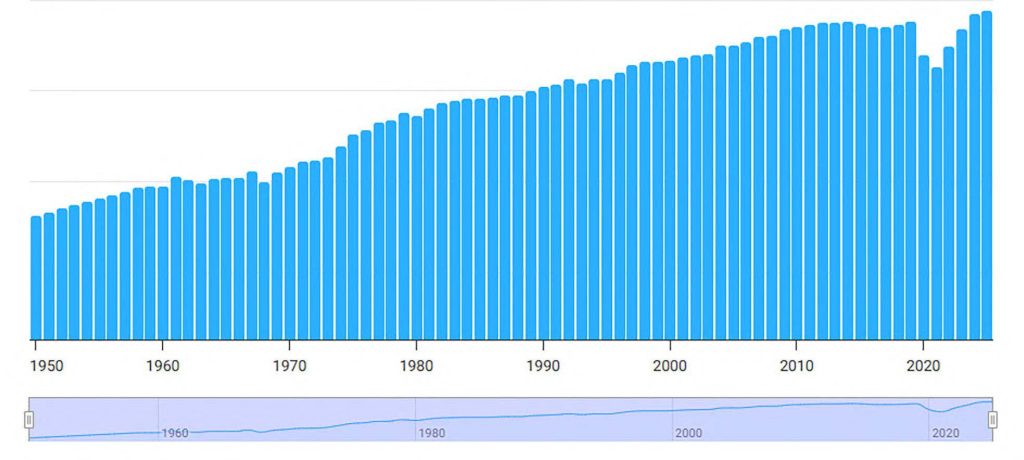
There are expected to be more cases of elder abuse as the older population increases over the next few decades (Table 2). This rise in the older population is due to steadily increasing life expectancy (Figure 1).8 In 2025, the life expectancy in the U.S. was 79.40 years, a 0.15-year increase from 2024.9,10
TABLE 2. Current and Project Elder Populations by State
| Population 2020 | Population Aged 65+ | Percent Change from 2020 to 2050 | ||||||
| State | Total Population per 100,000 | Population Aged 65+ per 100,000 | Percent of Total Aged 65+ | Projected 2030 per 100,000 | Projected 2040 per 100,000 | Projected 2050 per 100,000 | ||
| U.S. | 3,314.49 | 557.93 | 16.83 | 710.994 | 749.4722 | 758.8213 | 36.01 | |
| Alabama | 50.24279 | 8.84723 | 17.61 | 10.81269 | 11.12827 | 10.90261 | 23.23 | |
| Arkansas | 30.11524 | 5.28867 | 17.56 | 6.292567 | 6.330529 | 6.189348 | 17.03 | |
| Florida | 215.3819 | 45.68026 | 21.21 | 60.61127 | 67.78633 | 71.30848 | 56.10 | |
| Georgia | 107.1191 | 15.79289 | 14.74 | 21.42104 | 24.05294 | 24.67074 | 56.21 | |
| Kentucky | 45.05836 | 7.67159 | 17.03 | 9.359923 | 9.502082 | 9.180373 | 19.67 | |
| Louisiana | 46.57757 | 7.63143 | 16.38 | 9.217107 | 9.082425 | 9.09303 | 19.15 | |
| Mississippi | 29.61279 | 5.09561 | 17.21 | 6.164348 | 6.194124 | 5.962869 | 17.02 | |
| Missouri | 61.54913 | 10.77757 | 17.51 | 13.23339 | 13.0557 | 12.54987 | 16.44 | |
| North Carolina | 104.3939 | 17.89448 | 17.14 | 23.43858 | 25.68757 | 25.93711 | 44.94 | |
| Oklahoma | 39.59353 | 6.53078 | 16.49 | 7.868541 | 7.821278 | 7.867053 | 20.46 | |
| South Carolina | 51.18425 | 9.71951 | 18.99 | 12.625 | 13.62088 | 14.01236 | 44.17 | |
| Tennessee | 69.1084 | 11.79571 | 17.07 | 14.78307 | 15.5944 | 15.6768 | 32.90 | |
| Texas | 291.4551 | 39.21135 | 13.45 | 54.15924 | 62.10858 | 68.62719 | 75.02 | |
| Virginia | 86.31393 | 13.95291 | 16.17 | 17.92745 | 18.7517 | 18.59975 | 33.30 | |
| West Virginia | 17.93716 | 3.67015 | 20.46 | 4.082412 | 3.87171 | 3.528429 | -3.86 | |
FIGURE 1. US. Life Expectancy Trend from 1950 to 2025
Risk and Preventative Factors
There are several environmental and circumstantial factors that may increase a person’s vulnerability to elder abuse, many of which are compounded by the realities of aging. Table 3 identifies and provides examples for the three categories of elder abuse risk factors: individual, relationship, and social. One such example is the increased risk for a person with dementia. Dementia is a disease that primarily affects older adults, though early-onset dementia can occur.14 Currently, there are an estimated 6.7 million older adults living with dementia. Due to the mental decline caused by dementia, those with the disease are more vulnerable and more likely to experience one or more forms of abuse.15,16
Conversely, protective factors can counteract risk factors. Some known protective factors include a strong community and high emotional intelligence in both the victim and the caregiver.17,18 Using the same example of someone living with dementia, if that person were to be integrated into a strong social network prior to developing dementia, they are less likely to be socially isolated as the disease progresses, which in turn leads to higher levels of care oversight.19
TABLE 3. Risks Factors for Elder Abuse
| Individual | Relationship | Social |
| 1. Functional Dependence/Disability 2. Cognitive Impairment 3. Dementia/Alzheimer’s 4. Poor Physical Health 5. Pre-existing Intellectual Disabilities 6. Caregiver has a history of mental illness, substance abuse, or trauma 7. High-stress environment | 1. Past family conflict 2. Caregiver has high financial and emotional dependence upon a vulnerable elder 3. Caregiver lacks support 4. Caregiver struggles to establish or maintain prosocial relationships | 1. Social Isolation 2. Family Structure 3. Language Barriers 4. Understaffing/Lack of Qualified Staff Staff Burnout |
Adult Protective Services and Reporting
All states have Adult Protective Services (APS) as a means to report, investigate, and address adult abuse, neglect, and exploitation. APS is funded through a combination of federal, state, and local funds.21 Since 2024, APS programs have been required to provide at least two reporting mechanisms available 24 hours a day, seven days a week.22
States also have their own lists of mandated reporters for elder abuse—people who must report if they have a reasonable suspicion of elder abuse or neglect. These lists often include professionals such as physicians, nurses, behavioral health professionals, caregivers, clergy members, first responders, and, in some states, financial professionals.23
Barriers to Prevention and Defense
While federal and state frameworks addressing elder abuse are well established, implementation and enforcement face ongoing operational and structural challenges. These barriers affect detection, investigation, substantiation, and prosecution of abuse cases. Key constraints include underreporting, workforce and training limitations, and evidentiary challenges related to cognitive capacity
and consent.
Underreporting and Detection Gaps
Underreporting remains one of the most significant obstacles to preventing and addressing elder abuse. Although many professionals are mandated reporters, it is estimated that only 1 out of every 24 cases of elder abuse is reported to authorities.24 Financial exploitation is believed to be reported at even lower rates, with estimates suggesting that only 1 in 44 cases are brought to light.25
Underreporting limits policymakers’ ability to accurately assess the scope of the problem and allocate resources accordingly. Many prevention programs, APS staffing models, and prosecutorial resources are informed by reported case volume. When abuse is not reported, the true demand for services may be obscured, potentially constraining prevention planning and investigative capacity.
Financial consequences are also significant. A 2023 AARP analysis estimates older adults lose approximately $28.3 billion annually due to financial exploitation and abuse.26 Beyond economic loss, elder abuse and self-neglect are associated with increased mortality risk.27 Research indicates that certain forms of abuse, including neglect and financial exploitation, are correlated with lower survival rates compared to other forms.28
Victims may not report abuse due to fear of retaliation, shame, dependency on the perpetrator, or physical or cognitive limitations that impair communication. Professionals may fail to report due to high caseloads, limited training in recognizing non-physical forms of abuse, or uncertainty about reporting procedures. In rural areas and resource-constrained communities, limited access to specialized law enforcement or multidisciplinary investigative teams may further reduce detection rates.
Collectively, these factors create structural blind spots that can delay intervention and allow abuse to continue undetected. Table 4 outlines reasons why elder abuse is likely underreported.
TABLE 4. Reasons Elder Abuse is Underreported by Victims and Professionals
| Reasons a Victim Might Not Report | Reasons a Professional Might Not Report |
| Physical or Cognitive Impairment: Physical or cognitive limitations prevent communication or reporting | Inadequate Staffing: High workloads and understaffing in facilities lead to missed signs of abuse. |
| Shame and Fear: Overwhelming feelings of embarrassment or fear of physical retaliation | Assessment Barriers: Difficulty accurately interpreting signs of abuse or mistaking them for natural aging/conditions. |
| Dependency: Financial or physical reliance on the abuser for daily survival and care | Lack of Training: Unfamiliarity with mandatory reporting laws or the specific reporting process. |
| Protective Instincts: Emotional attachment or a desire to “save” the abuser from legal consequences | Fear of Consequences: Worrying about professional backlash, legal liability, or damaging relationships with colleagues. |
| Lack of Awareness: Not recognizing that certain behaviors (like psychological abuse) are illegal or reportable |
Workforce and Training Constraints
Prevention and response efforts depend heavily on trained professionals across health care, social services, financial institutions, and law enforcement. Variability in training requirements and workforce capacity can affect the identification and documentation of abuse.
Individuals with dementia or Alzheimer’s disease are nearly five times more likely to experience abuse.31 Diagnostic and cognitive assessment practices also vary. The Alzheimer’s Association reports that 22 percent of primary care physicians did not receive residency training specific to dementia diagnosis, and many who did report feeling underprepared.32 Yet 85 percent of people receive their dementia diagnoses from a non-dementia specialist.33
Given the growing population of older adults and the prevalence of cognitive impairment, workforce preparedness in screening, documentation, and referral processes plays a central role in early detection. Gaps in training or limited access to specialists may delay diagnosis, complicate documentation of cognitive decline, and affect subsequent investigations.
Similarly, law enforcement agencies and APS offices may face staffing limitations, particularly in rural jurisdictions. To combat this, all the CSG South member states allow interagency collaboration when investigating the abuse of a vulnerable adult.34 This can take the form of co-response teams, where law enforcement is accompanied by a social worker or someone trained to recognize elder abuse.
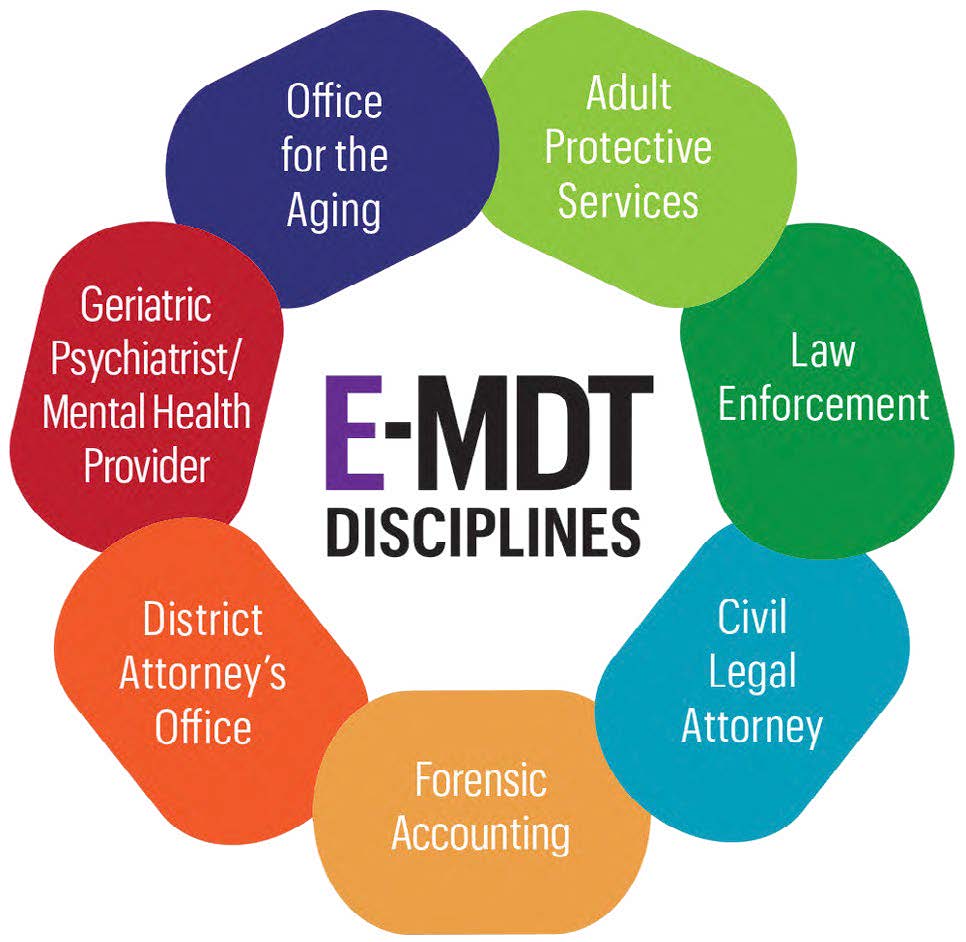
While states authorize multidisciplinary teams and interagency collaboration, resource constraints can affect the implementation and sustainability of these models. Figure 2 shows an example of what a multidisciplinary team addressing elder abuse may include.
FIGURE 2. Elder Abuse Multi-disciplinary Team Example
Evidentiary and Capacity Challenges
Substantiating and prosecuting certain forms of elder abuse—particularly financial exploitation—often requires establishing whether an older adult possessed the decision-making capacity to consent at the time of the alleged incident. Decision-making capacity refers to an individual’s ability to understand information, appreciate consequences, and communicate a choice. Capacity may fluctuate and can be affected by conditions such as dementia or other cognitive impairments.36
When contemporaneous medical documentation of diminished capacity is unavailable, determining whether a financial transaction or other action was voluntary can become more complex. In such cases, investigators and prosecutors may rely on circumstantial evidence, witness testimony, or retrospective assessments, which may present evidentiary challenges.
Obtaining formal cognitive evaluations during an active investigation can introduce additional time and cost considerations. Depending on jurisdiction and the assessment tool used, questions regarding admissibility or evidentiary standards may arise. In 2025, the National District Attorneys Association reported that gaps in statutory guidance addressing capacity-related issues and evidence-gathering procedures can limit prosecutorial effectiveness in elder abuse cases.37
While several states—including Florida, Kentucky, Louisiana, Tennessee, Texas, and West Virginia—require training in caring for people with limited capacity, few mandate that physicians receive training on diagnosing dementia and Alzheimer’s.38 Table 5 shows legislation from four states that mandate this type of training.
As the population aged 65 and older continues to grow, the intersection of cognitive decline, documentation practices, and evidentiary standards is likely to remain a central consideration in elder abuse prevention and enforcement efforts.
TABLE 5. State Legislation on Physician Dementia Diagnostic Training
| State | Measure (Year) | Summary |
| California | Senate Bill 0048 (2021) | This legislation expanded Medi-Cal benefits to include an annual cognitive health assessment for beneficiaries aged 65 or older who are not eligible for a similar Medicare assessment and requires that Medi-Cal providers complete specific training and use validated tools for the assessment. |
| Illinois | House Bill 2450 (2023) | This bill requires providers to complete one hour of dementia training every six years in order to maintain their license. |
| Massachusetts | House Bill 4116 (2018) | This mandated that physicians, physician assistants, and nurses complete a one-time training on the diagnosis and treatment of patients with Alzheimer’s and dementia. |
| Rhode Island | Senate Bill 0223 (2019) | This act requires licensed physicians and nurses to complete a one-time training (minimum of 1 hour of instruction) on the diagnosis, treatment, and care of patients with cognitive impairments, such as dementia. |
Federal Framework
The legal landscape protecting the rights and safety of elders in the United States is anchored by a triad of federal statutes. The Older Americans Act (OAA) of 1965 serves as the primary federal vehicle for delivering social and nutrition services, including home-delivered meals, transportation, and elder abuse prevention.39 The Nursing Home Reform Act (NHRA) of 1987 established national minimum standards of care and a legal “Bill of Rights” for residents in certified nursing facilities. Key protections include residents’ rights to be free from physical or chemical restraints and to participate in their own care plans. Failure to comply with NHRA’s standards jeopardizes a facility’s funding.40 The Elder Justice Act (EJA) of 2010 was the first comprehensive federal legislation specifically designed to address the abuse, neglect, and exploitation of older adults. A provision of the EJA requires long-term care facilities receiving at least $10,000 in federal funding to report reasonable suspicions of crimes against residents to both the Department of Health and Human Services and local law enforcement. Failure to report can result in significant monetary penalties, ranging up to $300,000 if the failure leads to further harm.41 Together, the Older Americans Act of 1965, the Nursing Home Reform Act of 1987, and the Elder Justice Act of 2010 form a comprehensive federal framework designed to prevent, detect, and prosecute elder abuse.
Southern State Efforts
Elder abuse is simultaneously a health, human services, and criminal law enforcement concern. Though all states have some type of law addressing elder abuse, several states in the CSG South region have recently been reviewing and revising their approach to handling elder abuse prevention and justice.
These systems are often comprised of medical training for recognizing declining cognitive ability and signs of abuse, Adult Protective Services and law enforcement officer training on elder abuse, and updating elder abuse definitions, prosecution standards, and relevant sentencing statutes.
What follows in Table 6 is an overview of these efforts from four states: Florida, Georgia, Tennessee, and South Carolina. These states were selected because they have each updated their elder abuse laws within the last three years, and those updates specifically deal with defining elder abuse, expanding elder and vulnerable persons’ protections against financial exploitation, and upgrading reporting systems. While other states in the CSG South region have looked to address this issue, the legislation chosen is meant to be reflective of potential approaches.
These policies are relatively recent, and their long-term impacts on elder abuse prevention and enforcement remain under
evaluation. Since Florida passed Senate Bill 0556, reports of elder financial exploitation increased by approximately 14 percent following implementation.42
Additionally, Georgia’s PACE program has shown improved health outcomes for older adults, with 93 percent of participants rating their care favorable and 11 percent fewer visits to the emergency department than other Medicare recipients.43 More research is necessary, but early indicators suggest these policies may be contributing to increased reporting and improved service delivery.
TABLE 6. Recent Southern State Legislation on Elder Abuse Prevention and Justice
| State | Measure (Year) | Summary |
| Florida | Senate Bill 0232 (2023) (Passed) | The legislation aims to prevent the exploitation of individuals aged 65 and older by defining exploitation conditions, establishing penalties, and allowing protective measures. |
| Senate Bill 0556 (2024) (Passed) | The legislation aims to protect older and vulnerable adults from financial exploitation by allowing financial institutions to delay transactions under suspicion, with specific procedures and immunity provisions. | |
| Senate Bill 0106 (2025) (Passed) | The bill amends Florida law to allow substitute service on unascertainable respondents in cases of exploitation of vulnerable adults, requiring an affidavit and holding disputed funds or property for 30 days. | |
| Georgia | Senate Bill 0084 (2023) (Passed) | This bill amends the Georgia Uniform Securities Act to protect elder and disabled adults from financial exploitation by mandating reporting, allowing transaction delays, and providing liability protections for compliant individuals. |
| House Bill 1078 (2024) (Passed) | This legislation introduces a new licensure exclusion for adult day centers and authorizes the Department of Community Health to establish the Georgia Program of All-Inclusive Care for the Elderly (PACE) as part of the state’s medical assistance program. | |
| House Bill 1123 (2024) (Vetoed) | This act would have required the establishment of multidisciplinary teams and an Elder Justice Coalition in Georgia to address abuse, neglect, and exploitation of disabled adults and elder persons, contingent upon funding, and mandates biannual reporting to state authorities. | |
| House Bill 0238 (2025) (Passed) | This bill requires the creation of a training course for responders to effectively handle situations involving at-risk adults with Alzheimer’s or dementia, developed in collaboration with the Division of Aging Services and approved by the Georgia Peace Officer Standards and Training Council. | |
| Tennessee | House Bill 0556/Senate Bill 1225 (2023) (Failed) | This legislation updates the notification process for convictions related to crimes against elderly and vulnerable adults, requiring notifications to be sent to the health facilities commission within ninety days. |
| House Bill 1248/Senate Bill 0756 (2024) (Passed) | This act authorizes a financial service provider, or an officer or employee of the provider, that has reasonable cause to suspect that an elderly or vulnerable adult is the victim or target of financial exploitation, to convey the suspicion to the TBI’s elder financial reporting mechanism; requires the TBI to create an elder financial exploitation reporting mechanism that accepts reports from financial institutions. | |
| South Carolina | House Bill 4556 (2024) (Failed) | This legislation would have established a registry for cases of abuse, neglect, or exploitation of vulnerable adults. |
| House Bill 3027 (2026) (In Committee) | This legislation exempts the Long-Term Care Ombudsman Program from reporting certain cases of vulnerable adult maltreatment to comply with federal confidentiality laws. | |
| House Bill 3617 (2026) (In Committee) | This bill mandates training for financial institution staff on identifying financial exploitation of vulnerable adults, allows vulnerable adults to designate trusted contacts, and requires reporting of suspected exploitation to authorities. |
Conclusion
Elder abuse remains a significant public health and public safety concern affecting older adults, families, and communities. Common themes emerging from state legislation are multidisciplinary teams and interagency collaboration, creating guardrails around financial transactions involving vulnerable adults, and increasing training for recognizing signs of elder abuse. These policies build upon previously established efforts to define and detect elder abuse.
End Notes
- U.S. Department of Justice. 2019. “About Elder Abuse.” Www.justice.gov. 2019. https://www.justice.gov/elderjustice/about-elder-abuse.
- U.S. Department of Justice. 2019. “About Elder Abuse.” Www.justice.gov. 2019. https://www.justice.gov/elderjustice/about-elder-abuse.
- World Health Organization. 2024. “Abuse of Older People.” World Health Organization. June 15, 2024. https://www.who.int/news-room/fact-sheets/detail/abuse-of-older-people.
- Weissberger, Gali H., Morgan C. Goodman, Laura Mosqueda, Julie Schoen, Annie L. Nguyen, Kathleen H. Wilber, Zachary D. Gassoumis, Caroline P. Nguyen, and S.Duke Han. 2020. “Elder Abuse Characteristics Based on Calls to the National Center on Elder Abuse Resource Line.” Journal of Applied Gerontology 39 (10): 073346481986568. https://doi.org/10.1177/0733464819865685.
- Nursing Home Abuse Center. 2010. “Emotional Elder Abuse – Signs of Emotional Elderly Abuse.” Nursing Home Abuse Center. 2010. https://www.nursinghomeabusecenter.com/elder-abuse/types/emotional-abuse/.
- Dong, XinQi, Ruijia Chen, and Melissa A. Simon. 2014. “Elder Abuse and Dementia: A Review of the Research and Health Policy.” Health Affairs 33 (4): 642–49. https://doi.org/10.1377/hlthaff.2013.1261.
- Henning-Smith, Carrie, Ingrid Jacobson, Dionne Bailey, Megan Lahr, Alexis Swendener, and Marguerite DeLiema. 2025. “Rural-Urban Differences in the Prevalence and Correlates of Elder Mistreatment.” Journal of Applied Gerontology, December. https://doi.org/10.1177/07334648251411579.
- Macrotrends. 2024. “U.S. Life Expectancy 1950-2024.” Macrotrends.net. 2024. https://www.macrotrends.net/global-metrics/countries/USA/united-states/life-expectancy.
- “U.S. Life Expectancy | Historical Data | Chart | 1950-2025.” 2025. Macrotrends.net. 2025. https://www.macrotrends.net/datasets/global-metrics/countries/usa/united-states/life-expectancy.
- “U.S. Life Expectancy | Historical Data | Chart | 1950-2025.” 2025. Macrotrends.net. 2025. https://www.macrotrends.net/datasets/global-metrics/countries/usa/united-states/life-expectancy.
- Bureau, US Census. 2024. “State Population by Characteristics: 2020-2021.” Census.gov. December 2024. https://www.census.gov/data/tables/time-series/demo/popest/2020s-state-detail.html.
- “National Population Projections | Cooper Center.” 2024. Coopercenter.org. July 22, 2024. https://www.coopercenter.org/national-population-projections.
- “U.S. Life Expectancy | Historical Data | Chart | 1950-2025.” 2025. Macrotrends.net. 2025. https://www.macrotrends.net/datasets/global-metrics/countries/usa/united-states/life-expectancy.
- CDC. 2024. “About Dementia.” Alzheimer’s Disease and Dementia. August 17, 2024. https://www.cdc.gov/alzheimers-dementia/about/index.html.
- National Institute on Aging. 2022. “What Is Dementia? Symptoms, Types, and Diagnosis.” National Institute on Aging. December 8, 2022. https://www.nia.nih.gov/health/alzheimers-and-dementia/what-dementia-symptoms-types-and-diagnosis.
- Dong, XinQi, Ruijia Chen, and Melissa A. Simon. 2014. “Elder Abuse and Dementia: A Review of the Research and Health Policy.” Health Affairs 33 (4): 642–49. https://doi.org/10.1377/hlthaff.2013.1261.
- Acierno, Ron, Melba A Hernandez-Tejada, Georgia J Anetzberger, Daniel Loew, and Wendy Muzzy. 2017. “The National Elder Mistreatment Study: An 8-Year Longitudinal Study of Outcomes.” Journal of Elder Abuse & Neglect 29 (4): 254–69. https://doi.org/10.1080/08946566.2017.1365031.
- Mueller, Emily A., Stacey A. Wood, Yaniv Hanoch, Yumi Huang, and Catherine L. Reed. 2020. “Older and Wiser: Age Differences in Susceptibility to Investment Fraud: The Protective Role of Emotional Intelligence.” Journal of Elder Abuse & Neglect 32 (2): 152–72. https://doi.org/10.1080/08946566.2020.1736704.
- Chang, E-Shien. 2021. “High Prevalence of Elder Abuse during the COVID-19 Pandemic: Risk and Resilience Factors.” The American Journal of Geriatric Psychiatry, January. https://doi.org/10.1016/j.jagp.2021.01.007.
- CDC. 2024. “Risk and Protective Factors.” Abuse of Older Persons. 2024. https://www.cdc.gov/elder-abuse/risk-factors/index.html.
- “Adult Protective Services: Background and Funding.” 2025. Congress.gov. 2025. https://www.congress.gov/crs-product/IF12917.
- “Federal Register :: Request Access.” n.d. Unblock.federalregister.gov. https://www.federalregister.gov/documents/2024/05/08/2024-07654/adult-protective-services-functions-and-grants-programs.
- “Mandated Reporting of Elder Abuse: What to Know – Benjamin Rose.” 2025. Benjamin Rose. February 17, 2025. https://www.benrose.org/resource/mandated-reporting-of-elder-abuse/.
- Mandated Reporter Training. 2023. “6 Reasons Why Elder Abuse Goes Unreported.” Mandated Reporter Training. September 7, 2023. https://mandatedreportertraining.com/resources/blog/6-reasons-why-elder-abuse-goes-unreported/.
- Nursing Home Abuse Center. 2010. “Elder Abuse Statistics – Statistics on Elderly Abuse over Time.” Nursing Home Abuse Center. 2010. https://www.nursinghomeabusecenter.com/elder-abuse/statistics/.
- Jilenne Gunther. June, 2023. AARP. The Scope of Elder Financial Exploitation: What It Costs Victims.
- Dong, XinQi. 2009. “Elder Self-Neglect and Abuse and Mortality Risk in a Community-Dwelling Population.” JAMA 302 (5): 517. https://doi.org/10.1001/jama.2009.1109.
- Burnett, Jason, Shelly L. Jackson, Arup K. Sinha, Andrew R. Aschenbrenner, Kathleen Pace Murphy, Rui Xia, and Pamela M. Diamond. 2016. “Five-Year All-Cause Mortality Rates across Five Categories of Substantiated Elder Abuse Occurring in the Community.” Journal of Elder Abuse & Neglect 28 (2): 59–75. https://doi.org/10.1080/08946566.2016.1142920.
- Mandated Reporter Training. 2023. “6 Reasons Why Elder Abuse Goes Unreported.” Mandated Reporter Training. September 7, 2023. https://mandatedreportertraining.com/resources/blog/6-reasons-why-elder-abuse-goes-unreported/.
- Schmeidel, Amy N., Jeanette M. Daly, Marcy E. Rosenbaum, Gretchen A. Schmuch, and Gerald J. Jogerst. 2012. “Health Care Professionals’Perspectives on Barriers to Elder Abuse Detection and Reporting in Primary Care Settings.” Journal of Elder Abuse & Neglect 24 (1): 17–36. https://doi.org/10.1080/08946566.2011.608044.
- Johnson, Mark J., and Howard Fertel. 2023. “Elder Abuse.” PubMed. Treasure Island (FL): StatPearls Publishing. 2023. https://www.ncbi.nlm.nih.gov/books/NBK560883/.
- Alzheimer’s Association. 2020. “Primary Care Physicians on the Front Lines of Diagnosing and Providing Alzheimer’s and Dementia Care: Half Say Medical Profession Not Prepared to Meet Expected Increase in Demands.” Alzheimer’s Association. Alzheimer’s Association. March 11, 2020. https://www.alz.org/news/2020/primary-care-physicians-on-the-front-lines-of-diagnosing-and-providing-alzheimer-s-and-dementia-care.
- O’Malley, Katherine. 2024. “Primary Care Physicians Should Be at the Heart of Treating Alzheimer’s.” STAT. March 27, 2024. https://www.statnews.com/2024/03/27/alzheimers-wave-needs-primary-care-physicians/.
- U.S. Department of Justice. 2016. “State Elder Abuse Statutes.” Www.justice.gov. April 8, 2016. https://www.justice.gov/elderjustice/elder-justice-statutes-0.
- NYS. 2023. “NYS E-MDT.” NYS E-MDT. 2023. https://www.nysemdt.org/participatingdisciplines.
- “Responding to Elder Abuse and Neglect: Mental Capacity and Consent – Nice Toolsets.” 2025. Nicenet.ca. 2025. https://www.nicenet.ca/tools/responding-to-elder-abuse-and-neglect-mental-capacity-and-consent.
- “Elder Justice Initiative – National District Attorneys Association.” 2025. Ndaa.org. 2025. https://www.ndaa.org/elder-justice-initiative.
- NCCDP. 2025. “NCCDP.” NCCDP. January 20, 2025. https://www.nccdp.org/federal-and-state-requirements-for-dementia-training-a-state-by-state-breakdown-of-current-guidelines/.
- Colello, Kirsten, and Angela Napili. 2025. “Older Americans Act: Overview and Funding.” Congress.gov. 2025. https://www.congress.gov/crs-product/R43414.
- Congress.Gov. 1987. “H.R.3545–100th Congress (1987-1988): Omnibus Budget Reconciliation Act of 1987.” Www.congress.gov. December 22, 1987. https://www.congress.gov/bill/100th-congress/house-bill/3545.
- Colello, Kirsten. 2020. “The Elder Justice Act: Background and Issues for Congress.” Congress.gov. June 15, 2020. https://www.congress.gov/crs-product/R43707.
- “FBI Highlights Growing Number of Reported Elder Fraud Cases ahead of World Elder Abuse Awareness Day | Federal Bureau of Investigation.” 2024. Federal Bureau of Investigation. 2024. https://www.fbi.gov/contact-us/field-offices/miami/news/fbi-highlights-growing-number-of-reported-elder-fraud-cases-ahead-of-world-elder-abuse-awareness-day.
- “Program of All-Inclusive Care for the Elderly (PACE) Updates.” 2025. Georgia Department of Community Health. 2025. https://dch.georgia.gov/programs/program-all-inclusive-care-elderly-pace-updates.