 DOWNLOAD
DOWNLOAD
A CSG South First Look
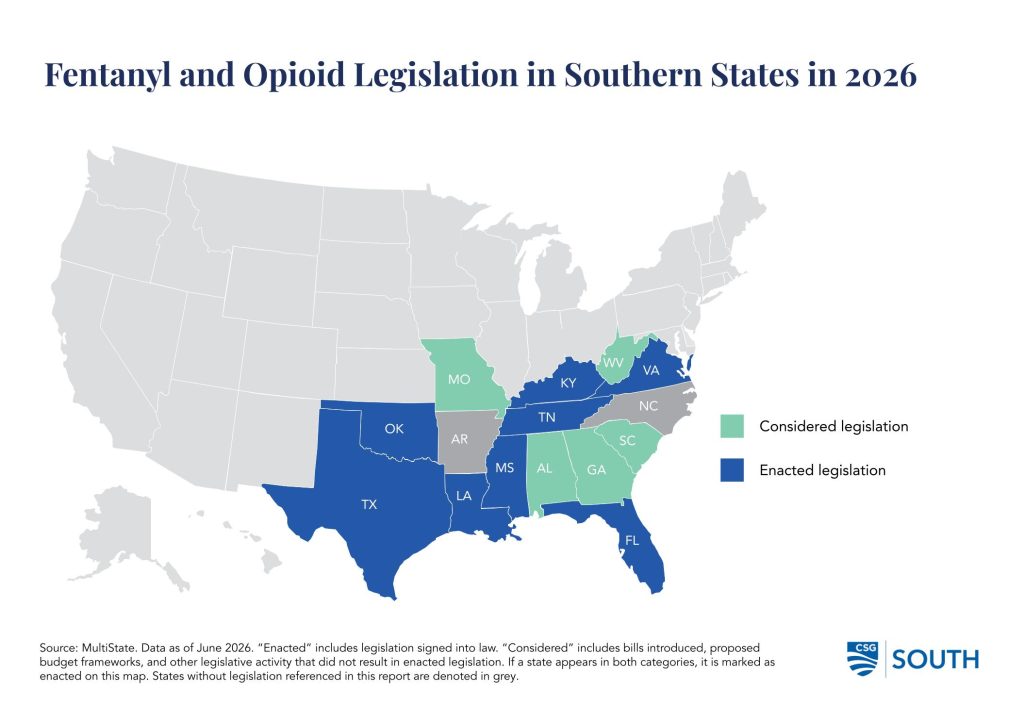
Southern states entered 2026 navigating an ongoing opioid crisis marked by illicitly manufactured fentanyl and counterfeit pills. This crisis brought federal and state health agencies to issue warnings regarding the potency and risks of synthetic opioids. In March 2026, the Tennessee Department of Health issued an alert following a rise in fatal overdoses associated with cychlorphine (a synthetic opioid). A month later, the Centers for Disease Control and Prevention (CDC) released a Health Advisory warning of medetomidine increasingly appearing in the illicit fentanyl supply and causing severe withdrawal symptoms. Given continued overdoses, Southern states have taken legislative action in response, focusing efforts on harm reduction, rescheduling, enforcement, education, and prevention. Below are some instructive examples of state legislation considered this year.
Legislative Activity in Southern States
Harm Reduction
Naloxone and other opioid antagonists, along with buprenorphine, are among the harm reduction tools states use to prevent lethal overdoses. States are pursuing policies to increase access to these tools. This year, Louisiana’s legislature enacted a law (LA HB 907) that grants criminal and civil immunity to people who prescribe, dispense, or distribute opioid antagonists past their labeled shelf life or act in good faith to administer an antagonist to people believed to be having an overdose. Additionally, Virginia enacted legislation (VA SB 257 / VA HB 795) requiring insurance coverage of prescriptions and opioid antagonists for overdose reversal on low-cost sharing tiers.
Regarding buprenorphine, southern states have implemented both regulatory and legislative action. Kentucky adopted regulations (KY 201 KAR 9:270) to establish professional standards to prescribe, dispense, and administer buprenorphine as an alternative opioid for substance use disorder treatment. Moreover, Tennessee enacted two laws that authorized healthcare providers to administer buprenorphine, on-site and without naloxone, for substance use disorder treatment (TN HB 1984) or for opioid use disorder if they are subcontracted with the Department of Corrections (TN SB 2549).
Southern states considered other harm reduction legislation. In 2026, Florida enacted legislation (FL HB 477) to decriminalize drug testing products, including test strips, used to detect fentanyl and other adulterants by excluding them from the definition of “drug paraphernalia.” Other states, including Kentucky (KY HB 680) and Mississippi (MS HB 448), introduced similar legislation, though both bills died in committee.
Rescheduling and Enforcement
States considered several avenues during this year’s legislative sessions to restrict unauthorized use of synthetic opioids and enforce penalties. A common approach was to add synthetic opiates and other fentanyl-related substances to the list of Schedule I substances. By enacting legislation to do so, states including Louisiana (LA HB 152), Mississippi (MS SB 2117), and Virginia (VA HB 558) further restricted their unauthorized use, distribution, or possession. Additionally, Alabama’s legislature opted to pass a resolution (AL HJR 281) urging the state’s Committee of Public Health to consider rescheduling the synthetic opioid cyclorphine as a Schedule 1 controlled substance.
State legislatures also considered bills to modify several criminal offenses concerning fentanyl. Kentucky enacted a law (KY SB 66) that includes the detection of fentanyl and other synthetic opioids in a driver’s blood as a DUI offense. Missouri’s legislature considered a bill (MO HB 1625) to lower the fentanyl quantity thresholds for existing drug trafficking offenses, and Georgia’s Senate adopted a bill (GA SB 604) to authorize the state Attorney General to prosecute violent crimes involving fentanyl trafficking. Additionally, Alabama’s (AL SB 309) and Kentucky’s (KY HB 750) legislatures considered bills to create new trafficking offenses based on different possession thresholds for fentanyl and cychlorphine, respectively.
Education and Prevention
Legislation focused on substance use education and prevention. During their regular legislative sessions, Texas (TX HB 3062) and Oklahoma (OK HB 1484) enacted legislation requiring fentanyl prevention and drug poisoning awareness education for students enrolled in public higher education institutions and grades 6-12, respectively. Similarly, legislation (SC S. 984) was introduced in South Carolina that would require all higher education institutions to provide opioid and fentanyl prevention education and mandate naloxone administration training for residence hall staff. West Virginia’s legislature considered a bill (WV HB 4655) that would extend “Laken’s Law” instruction, or mandatory education on fentanyl, opioid, and heroin awareness, prevention, and abuse given to students in grades six through twelve to students in grades three through five. Moreover, Missouri’s House of Representatives saw legislation (MO HB 3361) directing the state’s Task Force on Substance Abuse Prevention and Treatment to make recommendations on fentanyl education in schools.
Outside of student-focused education, states also considered bills that would support patient education and other statewide prevention efforts. Virginia enacted legislation (VA SB 308 / VA HB 794) to direct the Department of Health to develop a strategic plan to reduce opioid overdoses and deaths. Additionally, a bill (AL HB 364) in Alabama was introduced requiring providers to discuss the risks of addiction and overdose of opioids and other Schedule II drugs before issuing an initial and a third prescription. For patients under 18 years of age, the discussion would have to be held with their parent or guardian.