
A CSG South First Look
The Rural Health Transformation Program (RHTP) is a federal initiative created through the 2025 federal reconciliation bill to strengthen rural health systems. The program authorizes $50 billion in grant funding over five years. While the Centers for Medicare & Medicaid Services (CMS) sets oversight and reporting requirements, states have significant discretion to design plans around their own rural health priorities.
Program Structure and Funding
RHTP is structured as a state-driven grant program intended to support flexible investments, such as modernizing payment models, expanding telehealth, strengthening workforce strategies, and supporting community-based prevention, based on an approved state plan submitted to CMS.
As designed by Congress, $10 billion is available each fiscal year from 2026 through 2030. Half of each year’s funding is distributed equally across states with approved plans, and the remaining half is distributed at CMS’s discretion to support states with compelling initiatives or greater demonstrated need. Annual awards to states are informed by factors such as rural population and geography, existing infrastructure, provider and facility needs, and how closely state initiatives align with CMS program goals. CMS also requires ongoing reporting and monitoring tied to milestones and measurable outcomes.
CMS Priorities and Eligible Uses
CMS has identified priority areas that states can align to when requesting discretionary funding. Examples include:
- Evidence-based, measurable interventions to improve prevention and chronic disease management.
- Payments to health care providers for specified items or services.
- Consumer-facing, technology-driven solutions for prevention and chronic disease management.
- Training and technical assistance to adopt technology-enabled solutions in rural hospitals, including remote monitoring, robotics and artificial intelligence.
- Recruiting and retaining clinical workforce talent to rural areas, including multi-year rural service commitments.
- Technical assistance, software and hardware for significant information technology advances, including cybersecurity improvements.
- Efforts to right-size rural delivery systems across service lines (preventative, ambulatory, emergency, inpatient, outpatient and post-acute care).
- Support for opioid use disorder treatment services, other substance use disorder services and mental health services.
- Projects supporting innovative care models, including value-based arrangements and alternative payment models.
- Additional uses intended to promote sustainable access to high-quality rural health care, as determined by CMS.
Application Process and Timeline
CMS opened a single application window through a formal Notice of Funding Opportunity (NOFO). Each state was required to submit a single, consolidated application (joint or multi-state consortia were not permitted). Governors were able to designate a lead state agency or office responsible for statewide coordination and submission.
The application asked states to present a multi-year transformation plan that includes a rural health problem analysis, proposed interventions and any payment or delivery model changes, governance and accountability structures, measurable milestones and metrics, budget and funding requests, and plans for evaluation and public engagement. States were also asked to provide required assurances and reporting commitments for each fiscal year they expect to receive funds.
CMS released application instructions in mid-September 2025, set a formal application deadline of November 5, 2025, and approved state awardees in late December 2025. CMS has also indicated it does not plan to reopen the funding opportunity.
Funding Status and Near-Term Timeline
The initial phase of allocation is complete, and first-year award amounts have been announced to state agencies. The map and table below highlight relative funding awarded to southern states in the program’s first-year, with Texas being awarded the highest amount among southern states at $281.3 million.
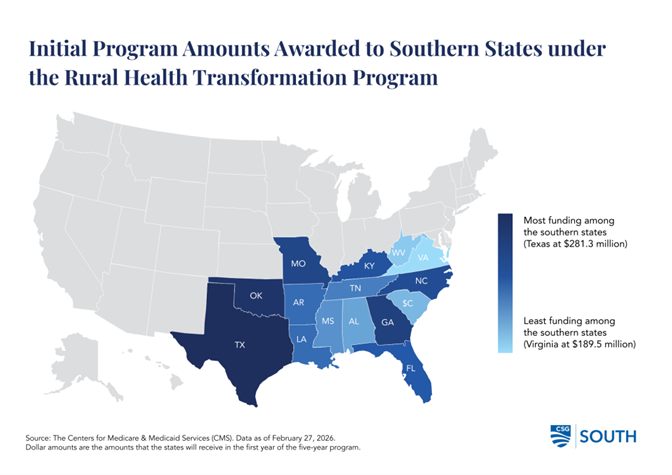
| State | FY26 Award |
|---|---|
| Alabama | $203.4 million |
| Arkansas | $208.8 million |
| Florida | $209.9 million |
| Georgia | $218.9 million |
| Kentucky | $212.9 million |
| Louisiana | $208.4 million |
| Mississippi | $205.9 million |
| Missouri | $216.3 million |
| North Carolina | $213.0 million |
| Oklahoma | $223.5 million |
| South Carolina | $200.0 million |
| Tennessee | $206.9 million |
| Texas | $281.3 million |
| Virginia | $189.5 million |
| West Virginia | $199.5 million |
However, the actual disbursement of these funds has not yet taken place. Recognizing the need for states to align their financial planning with these confirmed amounts, CMS provided states with the necessary time to review and revise their initial budgetary proposals. States were required to submit revised, finalized spending plans to align with their awarded total by January 30, 2026. Before the end of February 2026, CMS then either provided approval of those revised spending plans or issued requests for revisions. These revised budgets must accurately reflect the newly confirmed federal allocations and detail how the funds will be utilized to meet the program’s objectives. The final and crucial step before the funds are transferred is the official sign-off from the federal agency. It is expected that the majority of states will begin receiving the federal grant funds in the spring of 2026.
How States Approached Planning and Engagement
Because the program emphasizes community-rooted solutions, states and state associations have documented a range of mechanisms to solicit local input while drafting plans. Common approaches included listening tours and town halls, formal public comment processes, and engagement through advisory councils.
For example, Mississippi opened a public survey and convened a stakeholder forum to collect input; the state also requested quotes from consultants to support application development. Oklahoma, on the other hand, issued a “Request for Information” to collect ideas and feedback from rural residents, providers, and stakeholders. The state identified thematic focus areas including workforce development, technological innovation, regional partnerships, and health care access.
States generally organized their applications around five strategic goals:
- Innovative care (36 states),
- Sustainable access (45 states),
- Workforce development (47 states),
- Improving rural community health outcomes (34 states),
- Technological innovation (44 states)
Despite the freedom to tailor their plans, similarities exist. For example, most states are focusing on workforce development by leveraging high school programs to cultivate a pool of entry-level healthcare workers. Many are also allocating funds to enhance health information exchanges (HIE) between providers. While sharing common elements, each state’s plan ultimately features distinct aspects.
Key Questions Surrounding Implementation and Distribution of Funds
A central question is who holds authority to distribute federal grant funds. State approaches vary: many appear to centralize control within the governor’s administration or executive agencies, while others note constitutional or statutory requirements for legislative appropriation or seek legislative involvement in the allocation process.
Another common consideration is sustainability after federal funding ends in FY2030. Most states are proposing investments they believe can be maintained without ongoing state appropriations, though some are pairing short-term implementation activities with longer-term policy planning.
Finally, states are weighing how funds will flow to private entities and implementing partners. Mechanisms range from traditional procurement processes managed by a state agency to the creation of statewide governing entities responsible for grantmaking. In some cases, legislatures are seeking a formal role in these structures. Mississippi, Oklahoma, and West Virginia have all introduced legislation that would require agencies responsible for management of RHTP funds to make regular progress reports to the legislature on the program.
How State Governors Have Addressed RHTP
The extent to which the governors of each state have highlighted the creation of these plans and their ongoing work differs across states. Governors Ivey (R) of Alabama, Lee (R) of Tennessee, and Morrisey (R) of West Virginia have each used their State of the State addresses to call upon their state legislatures to enact crucial legislation. The governors seek to fully secure allocated state funding, a small part of which is contingent upon the adoption of specific policies. These contingent policies include removing restrictive certificates of need, joining interstate medical compacts, and expanding the scope of practice for mid-level practitioners. However, such conditions are not without merit as CMS has built these and other technical factors into its scoring criteria in determining states’ awarded amounts. In contrast, other governors who have given their State of the State addresses did not mention the RHTP at all.
Recent Developments and What to Watch Next
Following the award announcement, CMS formally established the Office of Rural Health Transformation to oversee program execution, serve as a dedicated point of contact for each state, and conducts ongoing monitoring against state milestones.
States had 30 days after receiving their award notifications to submit revised budgets reflecting actual award amounts. Those revised budgets must be approved by CMS before states can enter into a formal cooperative agreement, and this is the final step before federal dollars are transferred. As of early March 2026, most states are working through this process, meaning the practical deployment of funds is still weeks or months away for the majority of states (in spring of 2026). First-year funds must be fully expended by September 30, 2026, which may pose an administrative challenge for states given the tight timeline.
State legislatures have emerged as a key variable in the pace of implementation. In some states, executive agencies can proceed independently. In others, legislative action is required before federal funds can be spent. In West Virginia, for example, Governor Morrisey publicly warned in late February that delays in legislative authorization put the program’s timeline at risk.
Several states have moved quickly on the governance and workforce side while awaiting formal cooperative agreements. Alabama established a Rural Health Transformation Advisory Group by Executive Order, convening its first meeting in February, while Virginia and Georgia have both begun hiring dedicated program staff.
Looking ahead, subsequent year funding is not guaranteed at current levels. The discretionary half of each year’s $10 billion pool will be recalculated annually based on each state’s implementation progress and technical performance scores. This means that states that struggle to deploy funds, meet reporting and compliance expectations, or meet milestones in year one could see reduced allocations in coming years. Additionally, CMS is convening a state-only Rural Health Summit during its 2026 Quality Conference, where states will be expected to share early implementation lessons, challenges and feedback for CMS administration and oversight.